
What are new psychoactive substances?
There are multiple terms in use that refer broadly to new, novel or emerging drugs (1). This includes terms such as research chemicals, analogues, legal highs, herbal highs, synthetic drugs, designer drugs, bath salts, novel psychoactive substances, emerging psychoactive substances and new psychoactive substances. There is considerable variation in the terms used across countries and studies; to promote standardisation of terminology, the term ‘new psychoactive substances’ (NPS) has been adopted by the European Monitoring Centre for Drugs and Drug Addiction (EMCDDA), the United Nations Office on Drugs and Crime (UNODC), and the Australian Government Intergovernmental Committee on Drugs (2).
There remains no universally accepted definition of the term NPS, however they are most commonly defined as substances which do not fall under international drug controls, but which may pose a public health threat comparable to substances that are currently prohibited (3; pg. 6). However, the broadening of this definition in recent years means that, in practice, the term NPS can refer to psychoactive substances that: 1) are not scheduled under the 1961 United Nations Single Convention on Narcotic Drugs or the 1971 United Nations Convention on Psychotropic Substances; 2) are scheduled but have not previously been well established in recreational drug markets; or 3) have little literature relating to them (e.g. 3; pg. 6).
To date, approximately 900 NPS have been identified by the UNODC (4). It is unknown exactly how many (and which) of these NPS have been detected in Australia, however the UNODC has reported the total figure to be somewhere between 101 and 200 (see Figure 1).
Figure 1: Number of NPS reported by country, December 2018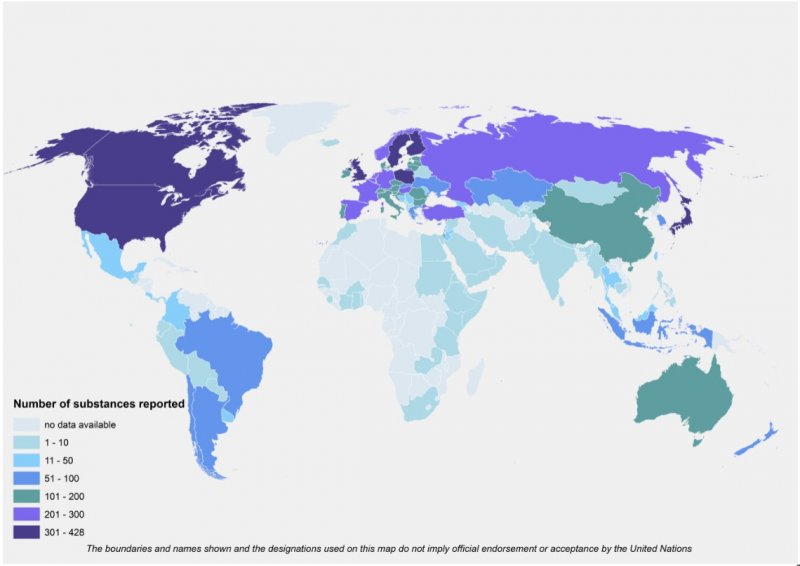
Source: United Nations Office on Drugs and Crime (4)
For the purpose of this paper, definitions of key NPS are provided in Table 1. For further information, including information on adverse effects, please refer to: https://ndarc.med.unsw.edu.au/sites/default/files/ndarc/resources/NDA073%20New%20Psychoactive%20Substances%20%28NPS%29.pdf; or https://yourroom.health.nsw.gov.au/publicationdocuments/quick-guide-ed3.pdf (chapter 15).
Table 1: Definitions of key NPS
Street name | Chemical name | Information on use and effects |
Phenethylamines | ||
2C series | - | Group of psychedelic phenethylamines, of which 2C-B is the most common. 2C-B has been described as a cross between LSD and ecstasy and is usually consumed in either powder or pill form. |
NBOMe series | - | Group of psychedelic phenethylamines that contain an N-methoxybenzyl group. The most common of the NBOMe series are derivatives of the 2C-series (but more potent), and include 25B-NBOMe, 25I-NBOMe and 25C-NBOMe. When deposited on blotter paper, LSD and NBOMe are virtually identical in appearance. |
Tryptamines | ||
DMT
| Dimethyltryptamine | Powerful hallucinogenic found in the seeds, bark, leaves or stem of various plants around the world. Consumed by many individuals as ayahuasca, however can also be synthesised into a crystalline form. |
Synthetic cathinones | ||
Mephedrone | 4-methyl-methcathin-one | A stimulant which is closely chemically related to amphetamines. Most commonly available as a powder, although it can also be pressed into pill form, and is usually snorted or ingested. |
Methylone | 3,4-methylenedioxy-N-methylcathinone | An entactogen and stimulant of the phenethylamine, amphetamine, and cathinone classes. Effects are primarily psychostimulant in nature. |
Synthetic cannabinoids | ||
Various (e.g. JHW-018, AB-CHMINACA, MDMB-CHMICA) | - | Substances that are functionally similar to delta-9-tetrahydrocannabinol (∆9-THC), the primary substance responsible for the psychoactive effects of cannabis. However, many of these substances have proven to be more potent than THC and are associated with more severe adverse effects and toxicity. |
Prevalence of NPS use in Australia
In Australia, national prevalence rates for NPS use were collected for the first time in 2013, through the National Drug Strategy Household Survey (NDSHS). The NDSHS is conducted on a triennial basis and collects data from the Australian residential population over 14 years of age. In 2013, 1.2% of the general population had used synthetic cannabinoids in the last 12 months, and 0.4% had used another NPS (5). In 2016, past-year synthetic cannabinoid use had declined significantly to 0.3% of the population, whereas other NPS use remained stable, also at 0.3% (6 ; Figure 2).
That is, despite the rapid growth of the NPS market, prevalence of use remains low among the general population.
Figure 2: Lifetime and past year use of NPS among Australians aged 14 years and older
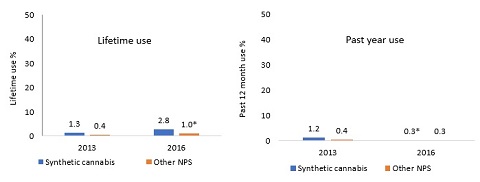
Source: Australian Institute of Health and Welfare (5, 6)
*significant change from 2013-2016
Is there a distinct group of NPS consumers?
Despite the low prevalence of NPS use, rates of use are elevated amongst vulnerable, high-risk populations. However, notwithstanding this evidence that NPS use is concentrated amongst existing illicit drug consumers (7, 8), and other disadvantaged groups (e.g. homeless, prisoners, mentally ill, people who inject drugs; 9, 10-13), concerns remain that ‘novice’ consumers may initiate NPS use, particularly given use of the internet as a means of supply. Indeed, the argument that NPS appeal to novice consumers has been used to advocate for their prohibition, regardless of their harm profile, on the premise of preventing normalisation of NPS use and transition into other illicit drug use (2).
In order to test the hypothesis of a distinct NPS consumer group, we used data from the 2013 NDSHS to identify the typology of Australian illicit drug consumers to determine if there was a group of exclusive NPS consumers (i.e. people who report use of NPS but no other illicit substances) - and if not, to determine which consumer ‘type’ was most likely to use NPS. Secondly, we were interested in comparing profiles across these subgroups, based on demographics and risk behaviours.
To address the first aim, we used latent class analyses and identified six types of Australian illicit drug consumers in the 2013 NDSHS (note: the NDSHS only breaks NPS into two groups - synthetic cannabinoids and ‘other’ NPS):
- Cannabis consumers (46%)
- Pharmaceutical consumers (21%)
- Ecstasy and cocaine consumers (19%)
- Amphetamine and cannabis consumers (7%)
- Polysubstance consumers (6%)
- Inhalant consumers (2%)
Our analyses confirmed that there is no distinct profile of exclusive synthetic cannabinoid or other NPS consumers in the Australian context, with very few participants (n=16; 5.7% of NPS consumers) reporting sole use of these substances. Rather, synthetic cannabinoid use was found to be highest among amphetamine and cannabis consumers (35%) and polysubstance consumers (31%), whilst other NPS use was highest among polysubstance consumers (31%). In short, our findingssupport the argument that most NPS consumers use a range of other illicit substances.
To address the second aim of this study, correlates of latent class membership were analysed using bivariate and multivariable multinomial logistic regression. To determine if the consumer groups with the highest rates of NPS use differed from other illicit drug consumers, the bivariate and multinominal regression models were run with both amphetamine and cannabis consumers and polysubstance consumers as the referent categories (these two groups had the highest probability of synthetic cannabinoid and other NPS use).
Detailed results can be found in the published article (https://www.sciencedirect.com/science/article/pii/S0376871618302345?via%3Dihub, or available upon request). However, to summarise, we found that polysubstance consumers (the group most likely to use NPS) were significantly younger than all other groups, and were generally more educated, with few differences in terms of income or socio-economic status. They were also more likely to engage in a range of drug-related risk behaviours, including undertaking dangerous activities while under the influence of drugs and/or alcohol (most commonly driving a motor vehicle), injecting drugs and hazardous alcohol consumption. This suggests that polysubstance consumers are a high-risk taking group, regardless of their NPS use, and as such, may not need specific NPS interventions. Rather, existing harm reduction messages surrounding drug use (e.g. the dangers of mixing substances, driving while under the influence, safe injecting practices) could be tailored for poly drug consumers more generally.
Amphetamine and cannabis consumers (the group most likely to use synthetic cannabinoids) were also quite young, however were more disadvantaged in terms of socio-economic status. They were more likely than all other groups to report trouble ceasing their drug use. Given that persistent desire or repeated unsuccessful attempts to quit is one of the markers of substance use disorder (14), it would seem that this is the group that may benefit most from treatment interventions. Indeed, existing treatment centres could incorporate the use of synthetic cannabinoids and other NPS into their screening/assessment processes, with treatment plans tailored accordingly. Amphetamine and cannabis consumers were also more likely than most other groups (excluding polysubstance and ecstasy and cocaine consumers) to engage in hazardous activity while under the influence of drugs and/or alcohol.
In summary, this study found no distinct profile of exclusive NPS consumers; rather the probability of synthetic cannabinoid and other NPS use was highest among amphetamine and cannabis consumers and polysubstance consumers. These groups reported the highest rates of drug-related harms (i.e. trouble ceasing use) and drug-related risk behaviours, respectively, suggesting that the use of synthetic cannabinoids or other NPS could be indicative of patterns of problematic drug use. These findings suggest that there may not need to be specialised NPS interventions or harm reduction messages; rather, they could be built into existing responses to drug use and targeted towards illicit drug consumers more generally.
Which specific NPS are being consumed in Australia?
Data from the NDSHS is limited by the fact it only separates NPS into two categories: synthetic cannabinoids and ‘other’ NPS. Thus, in order to obtain a more detailed understanding of patterns of NPS use in Australia, it is essential that this data be supplemented with data from sentinel or high-risk populations of illicit drug consumers. The Ecstasy and related Dugs Reporting System (EDRS) was the first project to start systematically collecting information on NPS use in Australia in 2010, whilst the Illicit Drug Reporting System (IDRS) started collecting information on NPS use in 2013. These are two Australian national monitoring studies funded by the Australian Government Department of Health, aimed at detecting emerging trends in illicit drug use, drug markets and drug-related harms. They have been conducted in all states and territories of Australia since 2000 and 2003 respectively, with samples consisting of people who regularly who ecstasy and/or other stimulant drugs (EDRS) and people who frequently inject drugs (IDRS) (see https://ndarc.med.unsw.edu.au/program/drug-trends for more details).
Data from these two studies show that rates of NPS use are elevated (but stable) among people who use illicit drugs (31% EDRS; 11% IDRS; Figure 3). Despite fluctuations in use of specific forms over the past eight years DMT and 2C-x remain the most commonly used NPS amongst the EDRS sample (Figure 5), whilst synthetic cannabinoids are the most commonly used NPS amongst the IDRS sample (Figure 4).
Figure 3: Past six month use of ‘any’ NPS among EDRS and IDRS participants, 2010-2018
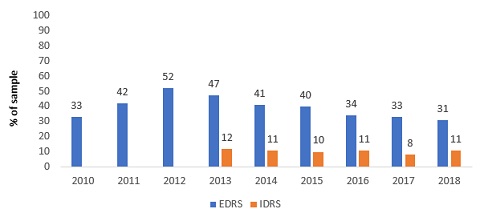
Source: Participant surveys from the EDRS and IDRS
Figure 4: Past six month of synthetic cannabinoid use among EDRS and IDRS participants, 2011-2018
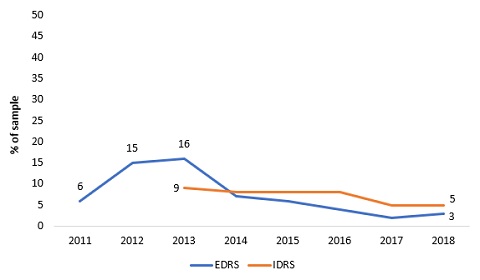
Source: Participant surveys from the EDRS and IDRS
Figure 5: Past six month use of other NPS among EDRS participants, 2010-2018
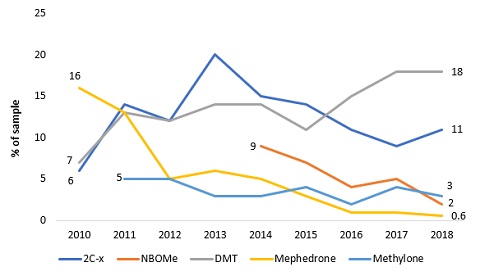
Source: Participant surveys from the EDRS and IDRS
Where do consumers obtain NPS from?
The rapid growth of the NPS market is often attributed to the expansion of online marketplaces, with NPS sometimes referred to as ‘internet drugs’. The expansion of these online drug markets have provided new opportunities for the supply and purchase of drugs, with internet sales of NPS now an international phenomenon and many online stores advertising worldwide delivery (15). However, despite these increased opportunities to obtain and supply substances, it remains unclear to what extent Australian consumers are using the internet for this purpose. We addressed this research gap using data from the 2016 EDRS and found that most NPS consumers (58%) nominated a friend as their main source for obtaining NPS in the past year. However, when comparisons were made across DMT, 2C-x, NBOMe and synthetic cannabinoid users it was found that NBOMe users were more likely to nominate a dealer (30%; p=0.045) or online marketplace (22%; p=0.010) as their main source, while synthetic cannabinoid users were more likely to nominate a shop (44%; p0.001) as their main source (Table 3). These findings demonstrate that, notwithstanding heterogeneity across consumers, most people who use NPS obtain these substances from in-person sources, such as friends and dealers.
Table 3: Source of NPS among EDRS participants, 2016
|
| Main NPS used in past year |
| |||
| Past year NPS consumers* n=296 %
| DMT (n=104) % (adjusted residuals) | 2C-x (n=59) % (adjusted residuals) | NBOMe (n=27) % (adjusted residuals) | Synthetic cannabis (n=23) % (adjusted residuals) | p value |
Main source (past year) % |
|
|
|
|
|
|
Friend | 57.5 | 66.7 | 69.5 | 48.1 | 52.2 | 0.146 |
Acquaintance | 4.4 | 5.9 | 5.1 | 0 | 4.3 | 0.645 |
Dealer | 17.0 | 17.6 (0.4) | 15.3 (-0.3) | 29.6 (2.0) | 0 (-2.3) | 0.045 |
Online# | 8.8 | 4.9 (-1.4) | 8.5 (0.3) | 22.2 (3.1) | 0 (-1.5) | 0.010 |
Shop | 8.8 | 0 (-2.0) | 0 (-3.1) | 0 (-1.2) | 43.5 (9.3) | 0.001 |
Other^ | 3.4 | - | - | - | - | - |
Source: Sutherland et al., 2017 (16)
*Includes DMT (n=104); 2C-x (n=59); NBOMe (n=27); synthetic cannabis (n=23); herbal highs (n=18); MXE (n=16); methylone (n=9); mephedrone (n=5); PMA (n=7); salvia divinorum (n=5); etizolam (n=5); mescaline (n=4); 5-Meo-DMT (n=2); LSA (n=1); datura (n=1); 3-MeO-PCP (n=1); 5-MAPB (n=1); ayahuasca (n=1); changa (n=1); kava (n=1); 5-Meo-MIPT (n=1); NBOH (n=1); phenibut (n=1); unknown (n=2)
^Includes workmates (1%); relatives (0.7%); home-made/grown (1.7%)
#Includes cryptomarkets (n=23) and surface web marketplaces (n=3); association remains significant even when surface web marketplaces are excluded from analysis
Note: significant findings bolded. Adjusted residuals only reported when p0.05 (adjusted residuals were used to analyse which cell differences contributed to the overall χ2 results. An adjusted residual score of greater than 2.0 or below -2.0 indicated that the cells differed significantly).