
Last year I had the good fortune to be awarded a Winston Churchill Travel Fellowship. This year in June and July I set off to investigate Managed Alcohol Programs in the UK and Canada. Before we delve into this novel service, let me outline some of the reasons why such a service can be beneficial.
Many homeless people are plagued by alcoholism. This group consumes over 20 standard drinks a day; often non-beverage alcohol (mouthwash) and drinks until unconscious. They place a high burden on hospitals and police and are subjected to assaults when drinking on the street. While abstinence from alcohol is preferred, it is unrealistic for a minority of chronic drinkers.
Consumption of non-beverage alcohol is widespread among street drinkers
In the UK, there were reports of alcohol based hand sanitizers being stolen from hospitals. This prompted one housing service to issue a warning of the dangers to clients. These gels are sought after for their high level of alcohol content despite being poisonous and extremely dangerous when consumed. Non-beverage alcohol includes rubbing alcohol, hand sanitizer and Listerine.
The Police and street drinkers
In the summer of 2010 and 2011 in Liverpool, residents and businesses were complaining about the anti-social behaviour of street drinkers in the city centre. The police grew tired of dealing with street drinkers, they would pour out their alcohol and move them on. This response was actively contributing to increased reports of begging as individuals lost their alcohol resorted to begging for money to buy more.
The Police also arrested the street drinkers, repeatedly, but this seemed fruitless as they would appear before the court, which was costly. Furthermore, it did not address the underlying cause. The Police realised it was costing a small fortune in staff costs and associated criminal justice costs which was not only unsustainable but inefficient.
A case study from the Police
The male offends predominately in Liverpool city centre and on the Wirral. In 2011, he was arrested for theft once, drunk and disorderly twelve times, breach of bail twice, court warrants for failing to attend court five times and breaching a dispersal order once. He was given an interim Anti-Social Behaviour Order in April 2011 for street drinking and arrested for breaching this three times. This was ratified to a full Anti-Social Behaviour Order and he has been arrested for breaching this 22 times. It was estimated that 500 police staff hours have been spent dealing with this individual.
Meanwhile in Canada, the inclement weather saw numerous homeless persons die from exposure during winter. A group of business associates, police and social services came together to work out how to deal with the homeless problem.
Managed Alcohol Programs (MAPs)
As a way of addressing this group's needs, the idea of Managed Alcohol Programs was trialled. MAPs are usually a residential service. Residents need to be assessed in order to join the Program. Workers dispense a regulated amount of alcohol - one unit - to clients every hour from 7.30am to 9.30pm, an average of 15 drinks a day. Some Programs allow residents to have two units at the beginning of the day and then one every hour after.
Examples of MAPs
Manchester's the Heavy Drinkers' project is a residential Managed Alcohol Program with one core house with 15 outlying houses. The core house has seven bedsits and seven one-bedroom flats with support workers available 24 hours a day. Residents in the outlying houses can call the office for assistance but the idea is they are to live independently as far as possible including monitoring their own alcohol intake.
Canada has five managed alcohol programs. In Ottawa, the Targeted Engagement and Diversion program (TED) has 12 beds for men and two for women. TED is placed within a larger housing complex where other residents include families with children. The rationale behind having a MAP incorporated into a regular housing building was that families drink alcohol at home and children are exposed to that. Some residents are in Opioid Substitution Treatment (OST) as well. There are 80 other residents at TED who are not in the MAP.
Also in Ottawa, the OAKS opened in 2010 and has 55 beds of which 10 are for the mentally ill. Some 15-20 residents have lived there since it opened.

MAP in Ottawa
The Drug Users Resource Centre in Vancouver opened in 2003 and provides a safe, supportive and welcoming space for drug users, including alcohol dependents. Their MAP is a day service where clients are provided with alcohol but they do not live on the premises. Over 200 clients visit each day. Services include a methadone clinic and primary health care. There are work and volunteer opportunities and an arts and cultural program.
There are strict criteria for joining a Managed Alcohol Program
Eligibility criteria include homelessness or at risk of it and struggling with long-term alcohol dependence. Before coming into a MAP, many folk were consuming 30 units of non-beverage alcohol a day. They are not interested or able to attain abstinence. They have a high frequency of visits to hospital and regular contact with the police.
In Ottawa, clients for the MAP are identified through TED, the targeted engagement and diversion program. At the Drug Users Resource Centre, potential clients join a drinkers' lounge every Friday for a few weeks where they are assessed for suitability to enter the MAP.
A range of staff work in MAPs
Staff members include mental health workers, social workers, in-house support workers, nurses and doctors.
Finding a suitable location of a MAP can be difficult
Most MAPs were located in light industrial areas and near main train stations as these were places where the target population congregated. It was necessary to spend a considerable amount of time negotiating with the local Council, businesses and home owners to resolve this problem. There was opposition in terms of NIMBYism so it essential to engage with the community to move the project forward. The Oaks, which is situated in a residential area, faced much opposition to its location.
Residents are long-term alcohol dependents with a history of trauma
Street drinkers are not just the old style "tramp in the doorway," today they include younger males, females, non-Anglo persons, Inuit, Aboriginal and persons with acquired brain damage, Foetal Alcohol Syndrome or PTSD. Every single client has experienced some sort of trauma. The MAP is an intervention to stabilise residents' drinking who are then in a position to deal with other issues.
Many residents have concurrent disorders; alcohol dependence and mental illness. Very heavy drinkers, who consume over 400 units of alcohol per week, have problems that require social and medical solutions rather than a policing one.
Dispensing alcohol
In Ottawa, a doctor determines the level of dosing which usually ranges from 5 to 7 oz. of alcohol an hour. Residents receive 12 units a day and they can have beer, wine or Vodka. Once the resident selects a particular type of alcohol, they must stay with it for the day, although they can change the type of alcohol the next day. A record is kept of the amount and time that alcohol is dispensed to each resident.
Clients and residents I met
Workers at each Centre allowed me to meet a number of their clients or residents. I was able to talk to them in private about their lives. The overwhelming message from these people was that they had been given a chance to rejoin society, to be valued and were happy that someone still cared for them. Most had spent many years in a downward spiral where they had endured some pretty tough times. All had been subjected to violence while on the street, most had been rejected by their families and many felt a sense of failure from being heavily dependent on alcohol. When asked about the programs and staff, everyone I spoke to was full of praise for the work of the Centre staff. All accepted the rules and supported the staff whenever possible.
Declan, an elderly Irish gentleman, was drinking 260 units of alcohol a week (6 bottles of wine a day) before entering the program and now drinks 125 a week in the program; less than half. He has a support plan which is outcome driven and reviewed every three months. Declan has psoriasis on his hands and feet and is waiting until he can go six weeks without alcohol in order to have the laser treatment. His daughter and a worker go to the bottle shop each week and buy his alcohol and cigarettes.
The views of staff
Without exception all staff were completely dedicated to their jobs. They had many stories to share about how clients had improved and rebuilt relationships with their families and friends. One confronting revelation was that some staff saw the MAP as palliative care and that some clients would never move on, rather this would make their final years more bearable than otherwise.
MAPs have good relationships with the police and ambulance services
All Centres reported that it was essential to work closely with the Police to operate MAPs. They also work closely with health centres, which means it is rare for an ambulance to be called and visits to the Accident and Emergency Department are genuine as staff filter the use of these services.

Ambulatory room in Ottawa
In Ottawa, the TED Centre accepts patients from Paramedics who enter their observation room rather than being admitted to hospital. They are observed for 24 hours. This approach has saved $2m in averted hospital costs. However, when MAP residents are transferred to hospital they still need to be maintained on alcohol, otherwise they will leave hospital. Several MAPs had an arrangement with the local hospital, which allowed workers to bring their doses of alcohol into them.
Rules vary across Programs
Some MAPs restricted drinking and smoking to residents' rooms, while others allowed residents to drink in communal areas but not in their rooms. The atmosphere in the MAPs does not have a party feel to it, even though everyone is drinking alcohol.
MAPs do more than just provide alcohol
Centres provide a range of services to their clients such as assisting clients to obtain Identification or birth certificates. Centres provide free food, laundry facilities, toiletries, snacks, coffee, local and long distance phone calls and computer access. The Canadian services provided acupuncture for the treatment of stress, trauma and addiction. These agencies also provided traditional food for indigenous clients such as seal, whale and moose. Activities include a walking group, cooking, gardening and a coffee morning. Other Centres provided a table tennis, a drama group, gardening and art classes. One Centre had a performance space available for clients to put on their own shows. Other services include a foot care and a wound care clinic. Staff monitor clients' liver function. At a MAP it can be the first visit to the doctor and dentist for many clients for some time.
Workers provide residents with work and volunteer opportunities and a daily job draw, which is paid. Residents can earn money by collecting bottles for recycling. The vast array of activities occupy the residents' time and helps them reducing their focus on drinking and alcohol consumption. Residents and clients are encouraged to have their family and friends visit and to engage in positive social interactions.
MAPs brewed their own alcohol
Several Centres had decided to brew their own alcohol. This decision was reached due to the amount of alcohol dispensed through MAPs each week. One Centre in Ottawa was spending $1,500 on alcohol every fortnight, or $39,000 per year. Given home brewing is labour intensive, it made sense to cajole residents to assist in the process.
The Oaks residents brew their own alcohol and dispense 810 gallons every 5 weeks for 55 people. It costs $5,000 a brewing kit, which is made up in 45-gallon drums

Home brewing at the Oaks Ottawa
Residents can progress from a MAP
Most Centres operate MAPs at two levels; providing 24-hour supervision in the main house and less supervision in outlying houses. At the main house, their alcohol consumption is managed very closely, with it being dispensed every hour during the day. At the outlying houses, residents live independently with off-site support and manage their own alcohol consumption. Staff work with people over a long period so they are able to manage their own alcohol consumption.
People improve when they join a Managed Alcohol Program
When residents arrive at a MAP, they are self-centred. "It is all about me, myself and I". As they progress, they are able to welcome others and are able to consider other people. They lose the chip on their shoulder and open up. There is a sense of community where residents learn to bond and to manage conflict, without violence. One woman was very aggressive with staff from a range of services but once she entered the MAP she stopped being aggressive.
Peer workers, residents who have progressed enough to carry out some duties at the Centres, are employed at MAPs. This serves to illustrate that change is possible and among people exactly like themselves.
Experience suggests that it takes three to five years to see any improvement in clients' brain function. A study on executive functioning found that clients had good verbal skills but responded poorly to stimuli and operated at the level of an eight year old. One person had 15 visits to a hospital over a one-month period and many interactions with the police. After joining the MAP, the person has had no hospital visits and very few interactions with the police.
MAPS are controversial
The notion of providing alcohol to 'alcoholics' is controversial. It is unsurprising that there would be community opposition to the placement of a MAP in their area. Managers of MAPs spoke of prolonged community consultation in order to establish the service and to counter resistance.
MAPs are an effective intervention
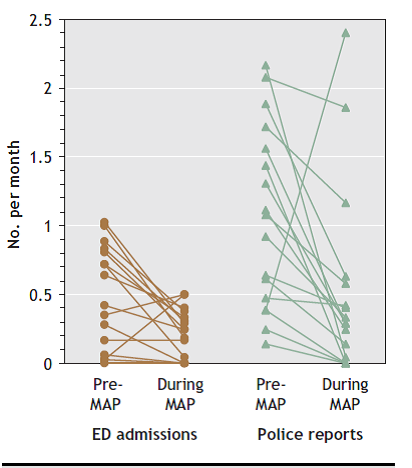
An evaluation found most residents wanted a regulated, a normal life. The female clients wanted to have friends and be able to eat a meal with others. A study of 17 adults in a MAP with an average age of 51 years had been dependent alcohol for an average of 35 years. After 16 months in the Program, their mean monthly visits to accident and emergency departments decreased from 13.5 to 8 (p=0.004) while Police encounters decreased from 18.1 to 8.8 (p=0.018) (See graph below). All participants reported less alcohol consumption. Staff noticed that residents had improved hygiene and compliance with health care (Podymow, 2006).
Graph Number of A & E and Police contacts pre and during the MAP
Conclusions
Homeless people have high rates of chronic illness, long hospital stays, increased mortality and contact with the police. The people who are homeless and drink heavily are stuck and unable to move out of their predicament. They need a comprehensive intervention to address mental health issues, alcohol and drug dependency issues, primary health care and their homelessness. Managed Alcohol Programs (MAP) are a novel service for homeless with severe and intractable alcohol dependence. MAP clients receive a regulated amount of alcohol at set times. MAPs operate in the UK and Canada and have led to reduced alcohol consumption, binge drinking, convulsions, visits to emergency departments and encounters with police.
Managed Alcohol Programs tend to be located in a light industrial area near a main train station, which are areas that most of the target population would frequent. Managed Alcohol Programs work well when there is a high level of co-ordination between services such as the police, health and housing.
Many clients are chronically ill and are dying from alcoholism. MAP improves their quality of life and while some take a break from drinking, few quit. MAP lessens the blow of alcohol on this group.
Winston Churchill Fellowship applications open 28 Feb 2016 and close 15 May 2016.